
In a recent study posted to the medRxiv* preprint server, researchers create a composite indicator for digital exclusion and a related toolbox.
 Study: Digital Exclusion as a barrier to accessing healthcare: A summary composite indicator and online tool to explore and quantify local differences in levels of exclusion. Image Credit: fizkes / Shutterstock.com
Study: Digital Exclusion as a barrier to accessing healthcare: A summary composite indicator and online tool to explore and quantify local differences in levels of exclusion. Image Credit: fizkes / Shutterstock.com
 *Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
*Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
Background
Digital exclusion in the United Kingdom is a growing issue, as it leads to marginalization and inequality. The coronavirus disease 2019 (COVID-19) pandemic and lockdown measures exacerbated inequalities in access to and use of digital tools.
Despite the increased incorporation of online services during the pandemic, such as medical appointments and social support services, there remains a lack of tools to measure local exclusion, thus making targeted interventions difficult.
Access, affordability, and ability are key factors in digital exclusion. Composite indicators such as poverty, national financial performance, human growth, and healthcare delivery can aid in analyzing the effects of policy change; however, they can also contribute to misinformation and poor policy planning and execution.
About the study
In the present study, researchers present the creation of a composite indicator and related online tool to assess the relative digital exclusion of each lower-layer super output area (LSOA) in the U.K. county of Lincolnshire.
The team provided measures regarding the time it takes to visit healthcare facilities using several modes of transportation. The composite measure includes Experian Mosaic indicators that account for relative disparities in degrees of digital competence, including the confidence and abilities individuals have in using online services.
The indicators reflecting different degrees of digital exclusivity were compiled for each LSOA in Lincolnshire. The variables were selected after a review of the literature and a series of interactions with stakeholders who were aware of socio-demographic and other issues that impede access to services in the local community.
Normalized and aggregated indicator variables were used. The D and E socioeconomic statuses (DER), guaranteed pension credit claims (GPC), internet (INT), low levels of activity (LAC), lack of qualifications (NQR), unemployment (UNP), transport (TRP), and Experian (EXP) are among the indicators utilized in the development of the digital exclusion indicator.
Small-area analysis was enabled by aggregating indicator variables at the different LSOA levels. A mean of the various component variables was employed for variables composing the INT, TRP, and EXP indicators.
Correlation plots and network diagrams were created to depict pairwise associations between the indicator variables integrated to build the composite indicator. This allowed the researchers to evaluate the extent of co-linearity among variables.
Factor analysis was used to establish weightings for the normalized indicators in the composite index. Loadings were calculated for all unobserved components or variables for all original indicators.
Study findings
The composite indicator and its development process have demonstrated potential relevance both in the U.K. and globally. The toolkit offers a web-based user interface for investigating regional differences in digital exclusion.
GPC, UNP, and DER were associated with a significant reciprocal association. LAC was associated with NQR, and the two only marginally correlated with DER.
A weak association between INT and TRP was also observed. EXP did not correlate with any indicator factors.
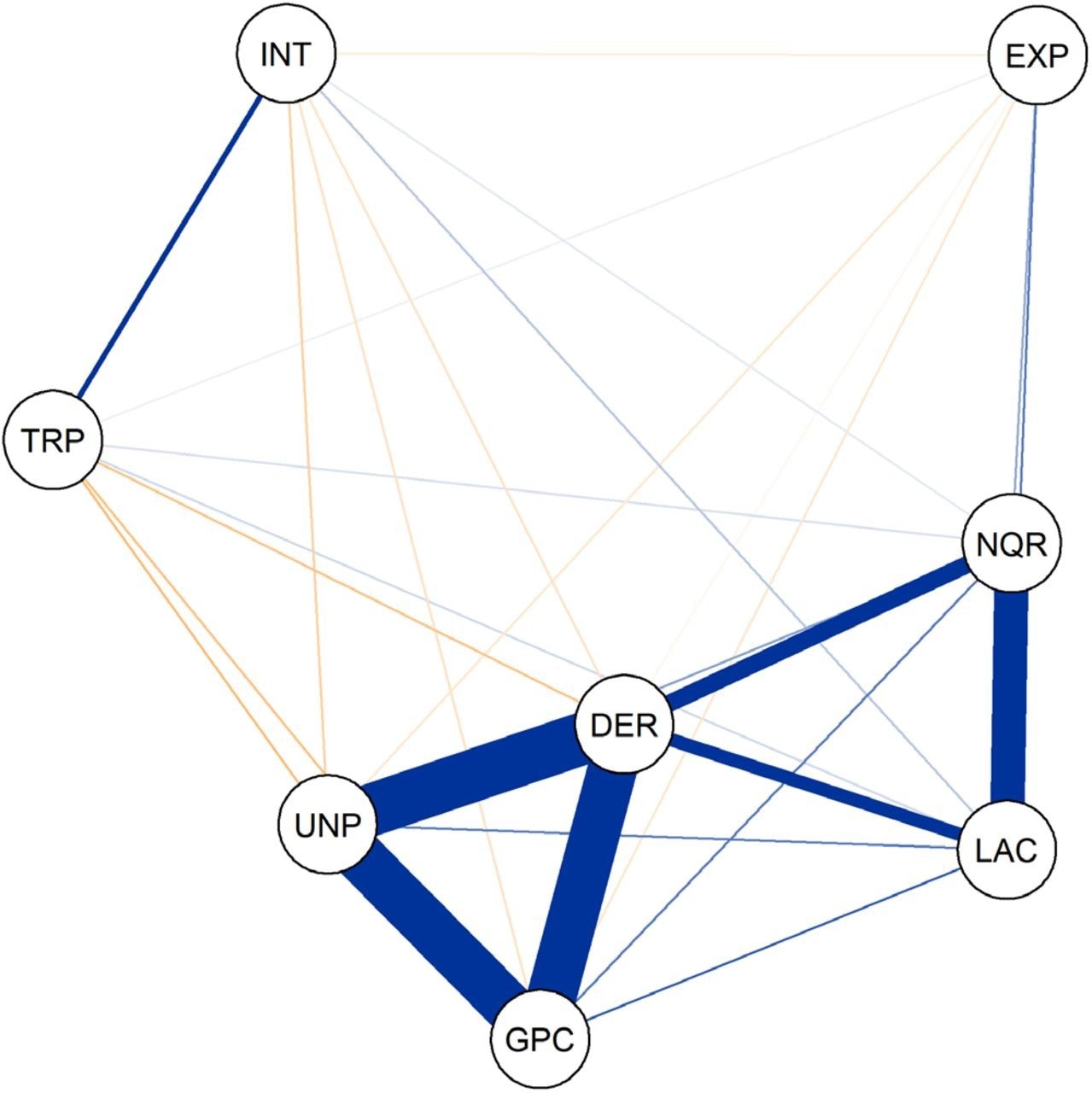 Correlation network diagram for the normalized indicator variables the thickness of the lines linking pairs of nodes indicates the strength of the correlations pair of variables.
Correlation network diagram for the normalized indicator variables the thickness of the lines linking pairs of nodes indicates the strength of the correlations pair of variables.
Socioeconomic disadvantage, inadequate academic credentials, a lack of exercise, and impediments to internet access were identified as underlying components. Lincolnshire’s easternmost coastline districts had the greatest levels of digital isolation, with large local variations within metropolitan areas including within Lincoln City or Grantham town.
The extraction of three factors that explained about 67% of the variation in the indicating variables was optimal.
The first component, which was primarily composed of four mutually associated variables of LAC, DER, GPC, and UNP, accounted for 31% of data variations. The second component, which was based on the NQR, LAC, DER, and EXP variables, explained 17% of the variation. The third component, which was based on TRP and INT, explained 16% of the variations.
Conclusions
Digital exclusion has serious consequences, including marginalization and inequity, especially for people who reside in geographically remote areas and have health-associated limits or impairments. The Digital Health Toolkit offers a new composite statistic adapted to the conditions of Lincolnshire, as well as an interactive dashboard that resources allocation choices and aims to combat digital exclusion.
Lincolnshire County Council has utilized the toolkit to sponsor a local charity’s service delivery focused on assisting individuals at an increased risk of being digitally excluded. Over 100 individuals in this community received gadgets, data SIM cards, and assistance in connecting to the internet. Using the toolkit, digital kiosks were installed at National Health Service (NHS) buildings in or near the county’s most digitally poor LSOAs.
*Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.







